NABL grants accreditation to medical testing laboratories in accordance with ISO 15189 “Medical laboratories-
requirements for quality and competence” The accreditation services to Medical Laboratories is currently given
in the following disciplines:
Medical Imaging- Conformity Assessment Body (MI-CAB)
The list of specific tests, types of tests or calibrations, PT Scheme, Reference Material for which a
laboratory is found competent is listed in scope of accreditation along with details like test methods, ranges,
CMC etc. The final content of the scope is recommended by the assessors and approved by NABL. It is
very important to note that scope don’t always include all the CAB’s capabilities. This is due either to the
CAB’s request to limit the scope, or because the assessors have not been able to affirm the CAB’s
competency in all areas for which the CAB was seeking accreditation. Capabilities that are not listed on the
scope of accreditation are not covered by the CAB’s NABL accreditation.
NABL Accreditation is currently given in the following fields and disciplines. The multi-disciplinary CABs shall
have to apply in relevant discipline separately depending upon to which discipline the scope belongs.
Medical imaging-conformity Assessment bodies (MI-CAB)
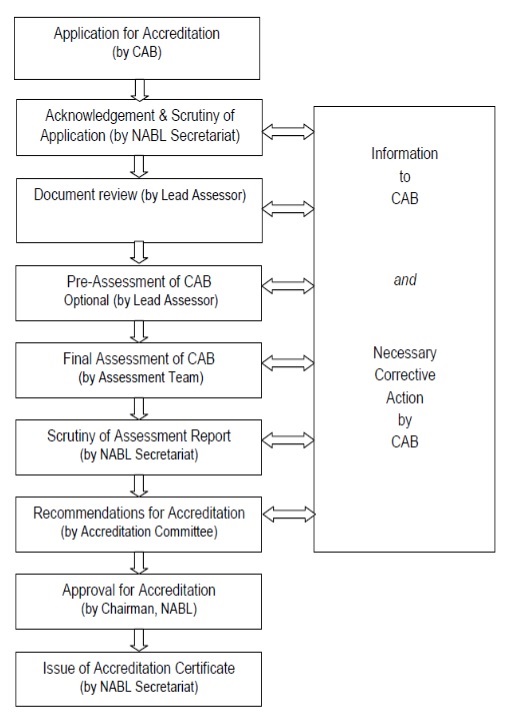
Preparations required by a CAB before applying for accreditation
quality manual submitted by the CAB is carried out by NABL Secretariat whereas the detailed
review is carried out by Lead Assessor.
The lead assessor informs NABL regarding the document review, indicating inadequacies (if
any). The CAB amends the relevant documents and also implements the management system
accordingly.
In case there are no inadequacies in the document review after satisfactory corrective action
by the CAB, a pre -assessment of the CAB is conducted by lead assessor appointed by NABL.
Since Pre-assessment is optional, CAB shall express its willingness in writing to undergo the
same. The CAB must ensure their preparedness by carrying out an internal audit and a
management review before the pre -assessment.
management system and its implementation and submits a report to NABL Secretariat.
After the CAB has taken corrective actions, NABL proposes constitution of an assessment
team. The team includes the lead assessor (generally same who is already appointed for preassessment),
the technical assessor(s)/ expert(s) in order to cover various fields within the
scope of accreditation sought. NABL may also nominate an observer. NABL seeks CAB’s
acceptance for the proposed assessment team and the CAB is free not to accept one or more
members of the proposed assessment team by giving specific reason(s) for their non –acceptance.
After the constitution of assessment team is finalized, NABL fixes dates for on-site
assessment in consultation with the CAB, the lead assessor and technical assessor(s)/
expert(s).
The assessment team reviews the CAB ’s documented management system and verifies its
compliance with the requirements of ISO/ IEC 17025: 2005/ ISO/IEC 17025:2017 or ISO
15189: 2012 or ISO/IEC 17043:2010 or ISO 17034:2016 whichever is applicable and relevant
specific criteria (wherever applicable) and other NABL policies. The documented
Management system, SOPs, work instructions, test methods etc. are assessed for their
implementation and effectiveness. The CAB’s technical competence to perform specific tasks
is also evaluated.
The assessment report contains the evaluation of technical manpower, all relevant material
examined, test witnessed including those of replicate testing/ measurement, compliance to
ISO/ IEC 17025: 2005/ ISO/IEC 17025:2017 or ISO 15189: 2012 or ISO/IEC 17043:2010 or
ISO 17034:2016 whichever is applicable and relevant NABL specific criteria. The nonconformities
if identified are reported in the assessment report. It also provides a
recommendation towards grant of accreditation or otherwise. The report prepared by the
assessment team is sent to NABL Secretariat. However, a copy of summary of assessment
report and copies of non-conformities if any, are provided to the CAB at the end of the
assessment visit.
Assessment of each declared Sample Collection Centre/ Facility (SCF) of a medical laboratory
will be done in each accreditation cycle. This may be done along with assessment of the
laboratory or separately as the case may be.
Scrutiny of Assessment Report
The assessment report is examined by NABL Secretariat and follow up action as required is
initiated. CAB has to take necessary corrective action on non – conformities/ concerns and
submit a report to NABL Secretariat within 30 days. NABL monitors the progress of closing of
non -conformities.
If any non-conformity is observed during the assessment of a Sample Collection Centre/
facility (SCF), the laboratory shall be asked to take corrective actions within 30 days time. In
case the laboratory fails to take corrective actions or there is a consistent system failure, an
appropriate and proportionate action against the laboratory will be taken.
After satisfactory corrective action by the CAB, the Accreditation Committee examines the
assessment report, additional information received from the CAB and the consequent
verification, if any.
In case the Accreditation Committee finds deficiencies in the assessment report, the NABL
Secretariat obtains clarification from the Lead Assessor/ Assessor/ CAB concerned. In case
everything is in order, the Accreditation Committee makes appropriate recommendations
regarding accreditation of the CAB to the Chairman, NABL.
All decisions taken by NABL regarding grant of accreditation are open to appeal by the CAB.
The appeal is to be addressed to the CEO, NABL.
Issue of Accreditation Certificate
When the recommendation results in the grant of accreditation, NABL issues an accreditation
certificate which has a unique number and QR Code, discipline, date of validity along with the
scope of accreditation.
The scope of accreditation for testing laboratory defines Discipline/ Group, materials or
products tested component, parameter or characteristic tested and Tests or Type of tests
performed and, where appropriate, the techniques, methods and / or equipment used.
The scope of accreditation for calibration laboratory defines Discipline/ Group, Measurand or
reference material, type of instrument or material to be calibrated or measured, and
Calibration or measurement method or procedure and Measurement range & additional
parameters where applicable and CMC in terms of Measurement uncertainty.The scope of accreditation for medical laboratory defines Discipline/ Group, Materials or
products tested component, Parameter or characteristic tested and Tests or type of tests
performed and, where appropriate, the techniques, methods and / or equipment used. The
annexure to theaccreditation certificate will also contain the details of recognized Sample Collection
Centres / Facilities associated.
The scope of accreditation for proficiency testing provider defines Proficiency Testing scheme/
Type of Proficiency testing item / Matrix and Measurand (s) or characteristic or type of
measurand or type of characteristic or analyte or parameter.
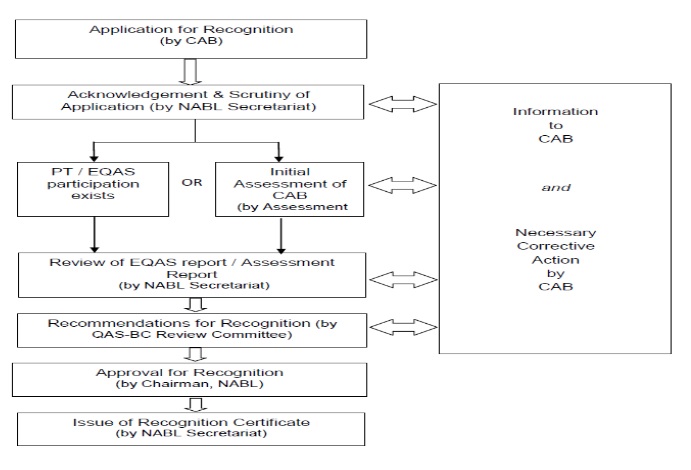
Quality Assurance Scheme for Basic Composite Medical Laboratories
(Entry Level)
Maintaining Accreditation
Surveillance and Re-assessment
NABL applies an assessment programme comprising of annual desktop surveillance during
each accreditation cycle of 2 years. At the end of the accreditation cycle, an on-site reassessment
is conducted covering representative scope of accreditation. The NABL
accreditation certificate is valid for a period of 2 years. NABL conducts annual Desktop
Surveillance which is aimed at evaluating continued compliance with ISO/IEC 17025:2005 or
ISO/IEC 17025:2017 or ISO 15189: 2012 or ISO/IEC 17043:2010 or ISO 17034:2016
whichever is applicable and relevant NABL specific criteria (wherever applicable) and
Policies. The types of assessments are given below: